
Pertactin-Positive Pertussis Strains: Antigen Composition and Clinical Relevance
In this article
Summary
Key points
- Bordetella pertussis incidence is rising globally despite high vaccination coverage, indicating continued disease transmission and epidemiological relevance1,2
- Pertactin, a 69‑kDa adhesin, plays a key role in bacterial attachment and immune evasion, contributing directly to pertussis pathogenesis5,6
- Anti-pertactin antibodies are strongly associated with protective immunity, supporting their role in enhancing bacterial clearance9
- Acellular pertussis vaccines contain up to 5 antigens (PT, FHA, PRN, FIM2/3), targeting multiple virulence factors10
- Multi-component (≥3 antigen) vaccines demonstrate higher efficacy (84–85%) (Range Across Studies) compared to 1–2 antigen formulations (59–78%)(Range Across Studies)11
- Acellular pertussis vaccines show lower reactogenicity than whole-cell vaccines, improving tolerability in clinical use11,12
- Pertactin-positive strains remain clinically relevant, supporting the continued importance of PRN inclusion in vaccine design3,4
Introduction
Bordetella pertussis, a gram-negative bacterium is the causative agent of pertussis (whooping cough), an acute and highly contagious respiratory infection that can lead to severe complications such as pneumonia, encephalopathy, and seizures. All age groups are affected by the disease, though newborns and infants under three months of age are most at risk for severe complications.1,2
Despite high vaccination coverage in developed countries and relatively low pertussis incidence for many years—especially during the COVID-19 pandemic—cases have begun to rise again, with outbreaks reported in several regions, a phenomenon referred to as the re-emergence of pertussis.1
One important factor contributing to the epidemiology of pertussis is the antigenic composition of circulating B. pertussis strains, particularly the presence or absence of key virulence-associated proteins such as pertactin.3 Pertactin-positive strains represent a biologically and clinically relevant category that continues to inform vaccine design, disease surveillance, and understanding of pathogen evolution.4
Pertactin and Its Role in Bordetella pertussis Pathogenesis
Pertactin (PRN) is a 69-kDa autotransporter adhesin that is highly conserved and expressed by Bordetella pertussis and other classical Bordetella species.5,6 It is regulated at the transcriptional level by a highly conserved two-component signalling system, the BvgAS regulon.6
Pertactin plays an important role in the pathogenesis of Bordetella pertussis, functioning not only as an adhesin at the bacterium–host cell interface but also contributing to resistance to neutrophil-mediated clearance. PRN participates in attachment through its arg-gly-asp motif to facilitate eukaryotic cell binding and invasion.5,6
- Role in respiratory infection: In respiratory infections, pertactin facilitates attachment to eukaryotic cells and may play an important role in colonisation of the respiratory tract.6
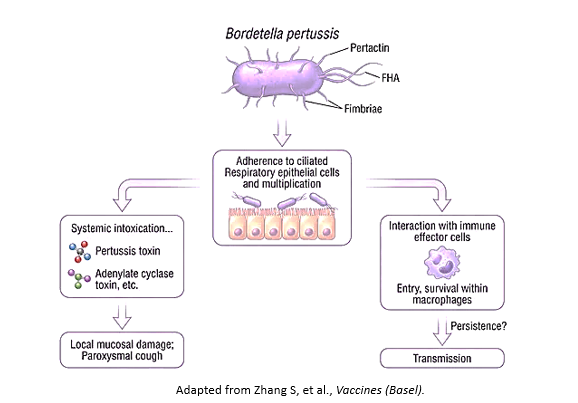
The key stages in pathogenesis of Bordetella pertussis are represented in Fig.17.
The schematic illustrates the progression of whooping cough, beginning with7:
- Bacterial attachment to the ciliated respiratory epithelium via adhesins such as Pertactin, FHA, and fimbriae.
- Followed by mucosal colonization and replication, leading to toxin-mediated damage.
- Pertussis toxin causes systemic effects, while adenylate cyclase toxin, tracheal cytotoxin, and dermonecrotic toxin damage the airway locally, resulting in paroxysmal cough and impaired mucociliary clearance.
Interactions with macrophages further promote immune modulation and bacterial persistence, supporting colonisation and transmission.
Immunogenic and Immunomodulatory Role of Pertactin
In addition to its role in bacterial adherence, pertactin contributes to immune recognition.
- Pertactin (PRN) is a highly immunogenic antigen with immunomodulatory functions, directly proportional to its expression in enhancing neutrophil-mediated phagocytosis.6,8 Antibodies against pertactin are produced following both natural infection and vaccination, and the protein is included in most acellular pertussis (aP) vaccines.6
Notably, only anti-pertactin antibodies—unlike those against pertussis toxin, fimbriae, or filamentous hemagglutinin—are key for B. pertussis phagocytosis, consistent with their correlation with protective immunity.9

Antigen Composition in Acellular Pertussis Vaccines10
Currently licensed pediatric and adult acellular pertussis (aP) vaccines contain up to five bacterial antigens, including pertussis toxoid (PT) and adhesion proteins such as filamentous hemagglutinin (FHA), pertactin (PRN), and fimbriae types 2 and 3 (FIM2/3). These antigens are selected due to their roles in disease pathogenesis and their effectiveness as immunological targets.
Clinical Significance of Pertactin-Containing Acellular Pertussis Vaccines11
Routine use of whole‐cell pertussis (wP) vaccines was suspended in some countries in the 1970s and 1980s because of concerns about adverse effects. Following this action, there was a resurgence of whooping cough. Acellular pertussis (aP) vaccines, containing purified or recombinant Bordetella pertussis antigens, were developed in the hope that they would be as effective but less reactogenic than the whole‐cell vaccines.
A Cochrane systematic review was conducted to assess the efficacy and safety of acellular pertussis vaccines in children and to compare them with the whole‐cell vaccines.
Study Design: Double‐blind randomised efficacy and safety trials
- Safety trial N= 136541
- Efficacy trial N= 46283
Table 1 demonstrates the comparative effectiveness of multi-component (≥3 antigen) versus low-component (1–2 antigen) acellular pertussis vaccines against typical and mild pertussis
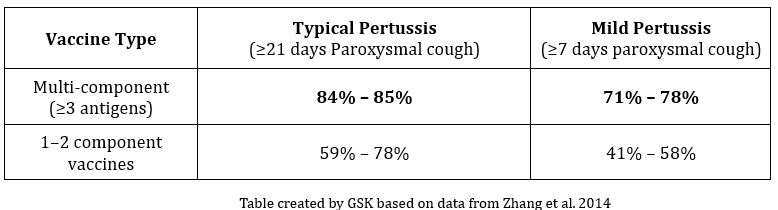
It is thus observed that multi-component (≥3 antigen) acellular pertussis vaccines achieve higher efficacy (84–85%) compared to 1–2 component vaccines, supporting the clinical value of broader antigenic coverage, including pertactin.
Additionally, it is noted,
- Multi‐component acellular vaccines are more effective than low‐efficacy whole‐cell vaccines.
- Most systemic and local adverse events were significantly less common with aP vaccines than with wP vaccines for the primary series as well as for the booster dose. Acellular pertussis vaccine is generally better tolerated with lower reactogenicity.12
The introduction of acellular pertussis (aP) vaccines in countries with a low uptake of whole-cell pertussis (wP) vaccines has led to a dramatic reduction in pertussis disease.13
Conclusion
Pertactin-positive Bordetella pertussis strains play a significant role in the epidemiology and pathogenesis of pertussis.3,4 As an important adhesin and immunogenic antigen, pertactin contributes to bacterial colonization and host immune recognition.5,6,8 Its inclusion in acellular pertussis vaccines highlights its importance as a target for protective immunity.8,10,11 Although the emergence of pertactin-negative variants has generated interest in pathogen evolution and vaccine pressure pertactin-positive strains remain clinically and epidemiologically relevant.4 Continued surveillance and research are essential to ensure that vaccination strategies remain effective against evolving B. pertussis populations.4
Key Safety Information14
Contraindications
Hypersensitivity to any active substance or excipient or formaldehyde, neomycin and polymyxin. Hypersensitivity after previous administration of diphtheria, tetanus, pertussis, hepatitis B, polio or Hib vaccines. Encephalopathy of unknown aetiology, occurring within 7 days following previous vaccination with pertussis containing vaccine. Postpone administration in acute severe febrile illness.
Special warnings and precautions
Carefully consider decision to give further doses if: temperature of ≥40.0°C (<48 hours of vaccination), not due to another identifiable cause; collapse or shock-like state (<48 hours of vaccination); persistent, inconsolable crying lasting ≥3 hours (<48 hours of vaccination); convulsions with or without fever, (<3 days of vaccination). Administer with caution in thrombocytopenia or a bleeding disorder. Do not administer intravascularly or intradermally. Rate of febrile reactions higher when co-administered with pneumococcal conjugate vaccine, or with measles-mumps-rubella-varicella vaccine; reactions mostly moderate (less than or equal to 39°C) and transient. Increased reporting rates of convulsions (with or without fever) and hypotonic hyporesponsive episode (HHE) were observed with concomitant administration of INFANRIX HEXA and Prevenar 13.
Special populations
HIV infection not a contraindication. Consider potential risk of apnoea and need for respiratory monitoring for 48-72h when administering primary immunisation series to very preterm infants (born ≤28 weeks of gestation) and particularly if history of respiratory immaturity.
Pregnancy and Lactation
INFANRIX HEXA is not intended for use in adults, adequate human data on use during pregnancy or lactation and adequate animal reproduction studies are not available.
Undesirable effects
Very Common- Appetite lost, crying abnormal, irritability, restlessness, somnolence, fever ≥38°C, local swelling at the injection site (≤50 mm), pain, redness
For the use only of a Registered Medical Practitioner or a Hospital or a Laboratory
References
- Leontari K, Lianou A, Tsantes AG, et al. Pertussis in Early Infancy: Diagnostic Challenges, Disease Burden, and Public Health Implications Amidst the 2024 Resurgence, with Emphasis on Maternal Vaccination Strategies. Vaccines (Basel). 2025;13(3):276. Published 2025 Mar 5.
- Rodrigues C, Bouchez V, Soares A, et al. Resurgence of Bordetella pertussis, including one macrolide-resistant isolate, France, 2024. Euro Surveill. 2024;29(31):2400459.
- Heininger U, Martini H, Eeuwijk J, et al. Pertactin deficiency of Bordetella pertussis: Insights into epidemiology, and perspectives on surveillance and public health impact. Hum Vaccin Immunother. 2024;20(1):2435134.
- Vodzak J, Queenan AM, Souder E, Evangelista AT, Long SS. Clinical manifestations and molecular characterization of pertactin-deficient and pertactin-producing Bordetella pertussis in children, Philadelphia 2007–2014. Clin Infect Dis. 2017;64(1):60–66.
- Leininger E, Roberts M, Kenimer JG, et al. Pertactin, an Arg-Gly-Asp-containing Bordetella pertussis surface protein that promotes adherence of mammalian cells. Proc Natl Acad Sci U S A. 1991;88(2):345-349.
- Inatsuka CS, Xu Q, Vujkovic-Cvijin I, et al. Pertactin is required for Bordetella species to resist neutrophil-mediated clearance. Infect Immun. 2010;78(7):2901-2909.
- Zhang S, Xu Y, Xiao Y. Revisiting Whooping Cough: Global Drivers and Implications of Pertussis Resurgence in the Acellular Vaccine Era. Vaccines. 2026; 14(1):35.
- Ma L, Dewan KK, Taylor-Mulneix DL, et al. Pertactin contributes to shedding and transmission of Bordetella bronchiseptica. PLoS Pathog. 2021;17(8):e1009735. Published 2021 Aug 4.
- Hellwig SM, Rodriguez ME, Berbers GA, van de Winkel JG, Mooi FR. Crucial role of antibodies to pertactin in Bordetella pertussis immunity. J Infect Dis. 2003;188(5):738-742.
- Dewan KK, Linz B, DeRocco SE, Harvill ET. Acellular Pertussis Vaccine Components: Today and Tomorrow. Vaccines (Basel). 2020;8(2):217. Published 2020 May 13.
- Zhang L, Prietsch SOM, Axelsson I, Halperin SA. Acellular vaccines for preventing whooping cough in children. Cochrane Database Syst Rev. 2014;(9):CD001478.
- Alghounaim M, Alsaffar Z, Alfraij A, Bin-Hasan S, Hussain E. Whole-Cell and Acellular Pertussis Vaccine: Reflections on Efficacy. Med Princ Pract. 2022;31(4):313-321.
- Poolman JT, Hallander HO. Acellular pertussis vaccines and the role of pertactin and fimbriae. Expert Rev Vaccines. 2007;6(1):47-56
- Infanrix Hexa Version: IFX-H/PI/IN/2025/01 Dated: 09-Dec-2025. https://india-pharma.gsk.com/media/a3hbdio3/infanrixhexa.pdf
GSK is not responsible for the third-party website content
Disclaimer
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website http://india-pharma.gsk.com/en-in/products/prescribing-information/ for full Product Information. Please report adverse events with any GSK product to the company at [email protected] ©2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).
CL Code: PM-IN-INH-WCNT-260015 | DOP: June 2026
For more information, please refer the following link
https://india-pharma.gsk.com/media/a3hbdio3/infanrixhexa.pdf
For Indian Healthcare Professionals Only
Key Safety Information
Contraindications
Hypersensitivity to any active substance or excipient or formaldehyde, neomycin and polymyxin. Hypersensitivity after previous administration of diphtheria, tetanus, pertussis, hepatitis B, polio or Hib vaccines. Encephalopathy of unknown aetiology, occurring within 7 days following previous vaccination with pertussis containing vaccine. Postpone administration in acute severe febrile illness.
Special warnings and precautions
Carefully consider decision to give further doses if: temperature of ≥40.0°C (<48 hours of vaccination), not due to another identifiable cause; collapse or shock-like state (<48 hours of vaccination); persistent, inconsolable crying lasting ≥3 hours (<48 hours of vaccination); convulsions with or without fever, (<3 days of vaccination). Administer with caution in thrombocytopenia or a bleeding disorder. Do not administer intravascularly or intradermally. Rate of febrile reactions higher when co-administered with pneumococcal conjugate vaccine, or with measles-mumps-rubella-varicella vaccine; reactions mostly moderate (less than or equal to 39°C) and transient. Increased reporting rates of convulsions (with or without fever) and hypotonic hyporesponsive episode (HHE) were observed with concomitant administration of INFANRIX HEXA and Prevenar 13.
Special populations
HIV infection not a contraindication. Consider potential risk of apnoea and need for respiratory monitoring for 48-72h when administering primary immunisation series to very preterm infants (born ≤28 weeks of gestation) and particularly if history of respiratory immaturity.
Pregnancy and Lactation
INFANRIX HEXA is not intended for use in adults, adequate human data on use during pregnancy or lactation and adequate animal reproduction studies are not available.
Undesirable effects
Very Common- Appetite lost, crying abnormal, irritability, restlessness, somnolence, fever ≥38°C, local swelling at the injection site (≤50 mm), pain, redness
For the use only of a Registered Medical Practitioner or a Hospital or a Laboratory
Abbreviated Prescribing information of INFANRIX HEXA [Diphtheria, tetanus, pertussis (acellular component), hepatitis B (rDNA), poliomyelitis (inactivated) and Haemophilus type b conjugate vaccine (adsorbed) Ph. Eur.]
ACTIVE INGREDIENT: Each 0.5 ml dose of reconstituted vaccine contains (i) Diphtheria toxoid ≥ 30 IU, (ii) Tetanus toxoid ≥ 40 IU, (iii) Bordetella pertussis antigens (Pertussis toxoid 25mcg, Filamentous Haemagglutinin 25 mcg, Pertactin 8 mcg), (iv) Hepatitis B surface antigen 10 mcg, (v) Inactivated Poliovirus [type 1 (Mahoney strain) 40 D-antigen unit, type 2 (MEF-1 strain) 8 D-antigen unit, type 3 (Saukett strain) 32 D-antigen unit), (vi) Haemophilus influenzae type b polysaccharide (polyribosylribitol phosphate, PRP) 10 mcg conjugated to tetanus toxoid as carrier protein (approximately 25 mcg).
INDICATION: Primary and booster vaccination of infants against diphtheria, tetanus, pertussis, hepatitis B, poliomyelitis and disease caused by Haemophilus influenzae type b.
DOSAGE AND ADMINISTRATION: Posology: The primary vaccination schedule should be administered according to official recommendations. Full-term infants or Preterm infants (≥24 weeks gestational age): 3-dose primary vaccination: interval of ≥1 month between primary doses. Booster dose ≥6 months after last priming dose; preferably ≤18 months of age. 2-dose primary vaccination: interval of ≥2 month between primary doses. Booster dose ≥6 months after last priming dose; preferably between 11-13 months of age. Administered according to official recommendations. The Expanded Program on Immunisation schedule (at 6, 10, 14 weeks of age) may only be used if hepatitis B vaccine given at birth. Safety and efficacy not been established in children > 36 months of age. Method of Administration: Deep intramuscular injection, preferably at alternating sites for subsequent injections.
CONTRA-INDICATIONS: Hypersensitivity to any active substance or excipient or formaldehyde, neomycin and polymyxin. Hypersensitivity after previous administration of diphtheria, tetanus, pertussis, hepatitis B, polio or Hib vaccines. Encephalopathy of unknown aetiology, occurring within 7 days following previous vaccination with pertussis containing vaccine. Postpone administration in acute severe febrile illness.
SPECIAL WARNINGS and SPECIAL PRECAUTIONS: Precede vaccination by review of medical history and clinical examination. Protective immune response may not be elicited in all vaccinees. Will not prevent disease caused by pathogens other than Corynebacterium diphtheriae, Clostridium tetani, Bordetella pertussis, hepatitis B virus, poliovirus or Haemophilus influenzae type b. However, Hepatitis D can be expected to be prevent. If any following events have occurred in temporal relation to receipt of pertussis-containing vaccine, carefully considered decision to give further doses of pertussis-containing vaccines: temperature of ≥40.0°C (<48 hours of vaccination), not due to another identifiable cause; collapse or shock-like state (<48 hours of vaccination); persistent, inconsolable crying lasting ≥3 hours (<48 hours of vaccination); convulsions with or without fever, (<3 days of vaccination). Appropriate medical treatment and supervision be available in case of rare anaphylactic event. Carefully weigh risk-benefit of immunising or deferring vaccination in infant or child suffering from new onset or progression of severe neurological disorder. Administered with caution in thrombocytopenia or a bleeding disorder. Do not administer intravascularly or intradermally. History of febrile convulsions, family history of convulsions or Sudden Infant Death Syndrome (SIDS) not a contraindication for use. Vaccinees with history of febrile convulsions should be closely followed up. Rate of febrile reactions higher when co-administered with pneumococcal conjugate vaccine, or with measles-mumps-rubella-varicella vaccine; reactions mostly moderate (less than or equal to 39°C) and transient. Increased reporting rates of convulsions (with or without fever) and hypotonic hyporesponsive episode (HHE) were observed with concomitant administration of INFANRIX HEXA and Prevenar 13. Antipyretic treatment should be initiated according to local treatment guidelines. Special populations: HIV infection not a contraindication. Expected immunological response may not be obtained in immunosuppressed patients. Can be given to preterm infants; however lower immune response been observed for some antigens. Consider potential risk of apnoea and need for respiratory monitoring for 48-72h when administering primary immunisation series to very preterm infants (born ≤28 weeks of gestation) and particularly if history of respiratory immaturity. Benefit of vaccination is high; vaccination should not be withheld or delayed. Interference with laboratory testing: Hib capsular polysaccharide antigen excreted in urine, positive urine test observed within 1-2 weeks. Interaction with other medicinal products and other forms of interaction: INFANRIX HEXA can be given concomitantly with pneumococcal conjugate vaccine (PCV7, PCV10 and PCV13), meningococcal serogroup C conjugate vaccine (CRM197 and TT conjugates), meningococcal serogroups A, C, W-135 and Y conjugate vaccine (TT conjugate), oral rotavirus vaccine and measles-mumps-rubella-varicella (MMRV) vaccine. Pregnancy and Lactation: INFANRIX HEXA is not intended for use in adults, adequate human data on use during pregnancy or lactation and adequate animal reproduction studies are not available.
ADVERSE EFFECTS: The following drug-related adverse reactions were reported in clinical studies (data from more than 16,000 subjects) and during post-marketing surveillance.
Very common (≥1/10): Appetite lost, crying abnormal, irritability, restlessness, somnolence, fever ≥38°C, local swelling at the injection site (≤50 mm), pain, redness.
Common (≥1/100 to <1/10): Nervousness, diarrhoea, vomiting, fever >39.5°C, injection site reactions, including induration, local swelling at the injection site (>50 mm).
Uncommon (≥1/1,000 to <1/100): Upper respiratory tract infection, cough, diffuse swelling of the injected limb, sometimes involving the adjacent joint, fatigue.
Rare (≥1/10,000 to <1/1,000): Lymphadenopathy, thrombocytopenia, anaphylactic reactions, anaphylactoid reactions (including urticaria), allergic reactions (including pruritus), collapse or shock-like state (hypotonic-hyporesponsive episode), bronchitis, apnoea, rash, angioedema, swelling of the entire injected limb, extensive swelling reactions, injection site mass, injection site vesicles.
Very rare (<1/10,000): Appetite lost, Convulsions (with or without fever), dermatitis.
OVERDOSE: No cases of overdose reported.
Version: IFX-H/API/IN updated on 10 May 2023.
Registered medical practitioners can refer company website www.gsk-india.com/product-prescribing-information.aspx for full Product Information.
Please report adverse events with any GSK product to the company at [email protected]
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website: india-pharma.gsk.com/en-in/products/prescribing-information/ for Full Product Information. Please report adverse events with any GSK product to the company at [email protected]. ©2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).