
Effect of a Single-Dose Varicella Vaccination Program: Findings from a Retrospective Cohort Study Highlight the Effectiveness of Two-Dose Strategies

In this article
Summary
Key points
- A large retrospective cohort study of 837,144 children (2011–2021) provides strong real-world evidence on varicella vaccination effectiveness3
- Single-dose varicella vaccination offers moderate protection ~72.5% VE (95% CI: 68.85-75.78) but does not adequately prevent breakthrough infections3
- Two-dose vaccination significantly improves protection, achieving ~90.3% (95% CI: 89.24-91.26) vaccine effectiveness3
- Breakthrough infection rates are higher with one dose (2.99 per 1,000) compared to two doses (1.06 per 1,000)3
- Two-dose schedules generate substantially stronger immune responses, contributing to reduced long-term infection risk3,5,7
- Despite high overall coverage (~91.8% receiving ≥1 dose), uptake of the second dose remains suboptimal3
- Introduction of vaccination programs has resulted in a marked decline in varicella incidence over time3
- Overall, findings support routine two-dose varicella vaccination for optimal and sustained protection3,7
Introduction
Varicella is a highly contagious disease caused by the varicella-zoster virus (VZV), a member of the alpha herpesvirus family. Following primary infection, VZV becomes latent in sensory ganglia and may reactivate years or decades later, resulting in herpes zoster (HZ).1 The virus is transmitted from person to person through direct contact or inhalation of aerosolized particles from vesicular fluid of skin lesions in acute varicella or zoster, and potentially via aerosolized respiratory secretions. The average incubation period is 14-16 days after exposure to a varicella or herpes zoster rash.2 Although most cases are mild to moderate, severe complications such as pneumonia, encephalitis, and hepatitis can occur, particularly in cases of secondary infection.1
Global and Indian Epidemiological Burden
- According to the World Health Organization (WHO), the global annual burden of varicella is estimated at approximately 140 million cases, with around 4.2 million severe complications requiring hospitalization and about 4,200 deaths. In the United States, prior to the introduction of the varicella vaccine (VarV), hospitalization rates were approximately 39.9 per 100,000 cases, with a mortality rate of 0.41 per million.3
- In India, between January 2015 and May 2021, a total of 1,269 chickenpox outbreaks comprising 27,257 cases were reported. Thirty-one deaths were confirmed, with the majority occurring in Bihar and Uttar Pradesh, while 19 states reported no deaths. Seasonally adjusted trends indicated that case numbers peaked during January to March.4
Evolving Vaccination Strategies
Implementation of the one-dose varicella vaccination program in the United States (1995-2005) resulted in significant declines in disease incidence, hospitalizations, and mortality. However, outbreaks persisted in school settings despite high one-dose coverage (>80%). Evidence from clinical trial demonstrated that a two-dose regimen elicited approximately 12-fold higher immune responses compared to a single dose, leading to a threefold reduction in breakthrough varicella over 10 years.
Based on these findings, the Advisory Committee on Immunization Practices (ACIP) recommended a routine two-dose varicella vaccination schedule for children aged 4–6 years in 2006.5
The Indian Academy of Pediatrics (IAP) Advisory Committee on Vaccines and Immunization Practices (ACVIP) recommends a two-dose varicella vaccination schedule, with the first dose administered at 15 months and the second dose administered at 18–24 months (preferably 3–6 months after the first dose).6
Efficacy of a 2-dose versus 1-dose varicella vaccine3
A retrospective study was conducted to evaluate the long-term efficacy of the two-dose varicella vaccine and to analyze its influencing factors.

Study design and population
Study Design: Retrospective observational cohort study
Study Period: 2011–2021
Sample Size: 837,144 children
Exposure Groups: Unvaccinated, One-dose vaccinated, Two-dose vaccinated
Follow-up: Long-term follow-up using existing records
Clinical outcomes
Characteristics of the subjects and vaccination rate
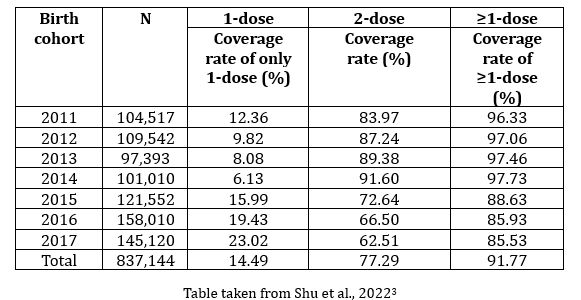
Across the 2011-2017 birth cohorts, data demonstrate high overall vaccination uptake, with progressive improvement in timing and interval of the two-dose schedule. While early cohorts showed strong transition to two-dose coverage, later cohorts experienced a decline in second-dose uptake, highlighting potential gaps in completing the full vaccination schedule.
Annual infection rate of different birth cohorts from 2011 to 2021
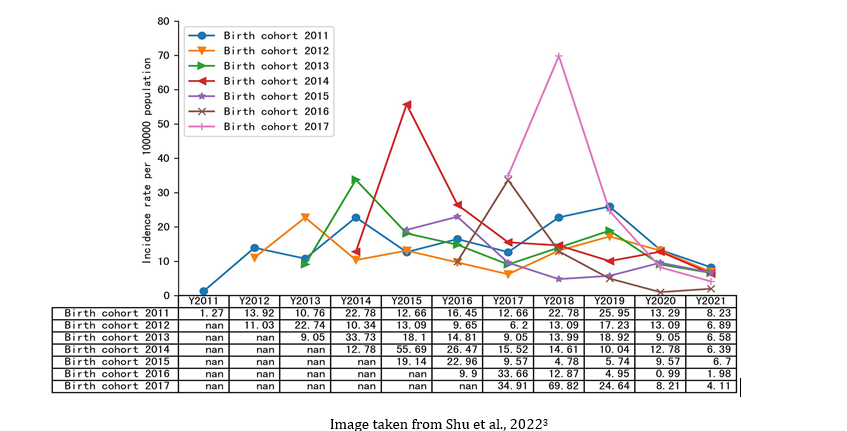
Across the 2011–2017 cohorts, varicella incidence was initially moderate and tended to rise in the first year of life before declining thereafter. A marked reduction was observed after 2020, with very low incidence across all cohorts by 2021, indicating effective disease control likely due to vaccination.
Breakthrough infection rate and the vaccine effectiveness
Birth cohort |
Vaccination status |
Breakthrough infection rates (1/1,000) |
VE (95%CI) |
P |
|
2011 |
Unvaccinated |
1.0 |
||
1-dose |
7.9 |
74.92 (67.22–80.80) |
<0.001 |
|
2-dose |
2.6 |
91.80 (89.73–93.45) |
<0.001 |
|
|
2012 |
Unvaccinated |
|||
1-dose |
5.48 |
85.86 (80.65–89.67) |
<0.001 |
|
2-dose |
1.37 |
96.48 (95.48–97.26) |
<0.001 |
|
|
2013 |
Unvaccinated |
|||
1-dose |
8.26 |
77.64 (69.11–83.81) |
<0.001 |
|
2-dose |
1.28 |
96.58 (95.46–97.42) |
<0.001 |
|
|
2014 |
Unvaccinated |
|||
1-dose |
8.56 |
82.49 (75.59–87.44) |
<0.001 |
|
2-dose |
1.05 |
97.88 (97.20–98.39) |
<0.001 |
|
|
2015 |
Unvaccinated |
|||
1-dose |
1.7 |
67.97 (51.65–78.78) |
<0.001 |
|
2-dose |
0.67 |
87.41 (82.24–91.07) |
<0.001 |
|
|
2016 |
Unvaccinated |
|||
1-dose |
0.72 |
82.91 (72.80–89.27) |
<0.001 |
|
2-dose |
0.3 |
92.75 (89.16–95.15) |
<0.001 |
|
|
2017 |
Unvaccinated |
|||
1-dose |
0.87 |
87.32 (81.10–91.50) |
<0.001 |
|
2-dose |
0.3 |
95.66 (93.45–97.12) |
<0.001 |
|
|
Total |
Unvaccinated |
|||
1-dose |
2.99 |
72.53 (68.85–75.78) |
<0.001 |
|
2-dose |
1.06 |
90.31 (89.24–91.26) |
<0.001 |
Table adapted from Shu et al., 20223
The breakthrough infection rate was higher with one dose (1.95 per 1,000 person-years) compared to two doses (0.61 per 1,000 person-years). Children receiving only one dose had significantly more infections than those with two doses. Overall, vaccine effectiveness was substantially greater with two doses (90.31%) than with a single dose (72.53%), demonstrating superior protection of the two-dose regimen.
Conclusion
Evidence from retrospective cohort study demonstrates that while a single-dose varicella vaccination program provides moderate protection and reduces disease burden, it is insufficient to fully prevent breakthrough infections and transmission.3 In contrast, the two-dose vaccination strategy offers significantly higher and sustained effectiveness, markedly lowering breakthrough infection rates and overall incidence of varicella.3 The findings consistently show higher-level vaccine effectiveness with two doses (~90%) compared to one dose (~72%), along with improved long-term disease control.3 Recent updates in the 2025 WHO position paper on varicella vaccines also highlight evidence supporting the higher immunogenicity and effectiveness of two-dose varicella vaccination strategies.7 Despite high overall vaccination coverage, gaps in completion of the second dose in later cohorts highlight the need for strengthening adherence to the full immunization schedule. Overall, the study strongly supports the implementation and maintenance of a universal two-dose varicella vaccination program for optimal and durable protection.3
Key Safety Information8
Contraindications:
Hypersensitivity to any active substance or excipient or neomycin. or varicella vaccine. Primary or acquired immunodeficiency who have total lymphocyte count <1200 per mm3 or other evidence of lack of cellular immune competence or subjects receiving immunosuppressive therapy (including high dose corticosteroids).
Pregnancy:
Avoid pregnancy for 1 month following vaccination.
Special warnings and precautions:
Postpone administration in acute febrile illness. Syncope (fainting) can occur following, or even before any vaccination, with adolescents, as a psychogenic reaction to injection. Avoid all contact with pregnant women susceptible to varicella (especially during first trimester pregnancy) and with high risk for developing severe varicella, especially when person vaccinated develops skin eruption within 2 to 3 weeks of immunization. To reduce infection risk of high-risk subjects, non-immune persons living in close contact with varicella patients or high-risk patients should be vaccinated. A decision should be made either to discontinue breastfeeding or to abstain from vaccination with VARILRIX, taking into account the benefit of breastfeeding for the child with regard to the benefit of prophylaxis against Varicella for the woman.
Undesirable effects:
Very common- redness, pain at the injection site.
For the use only of a Registered Medical Practitioner or a Hospital or a Laboratory
References
- Li Y, Xu F, Liu M, Teng S, Liang F, Wang F. Effectiveness of two-dose vs. one-dose varicella vaccine in children in Shanghai, China: a prospective cohort study. Front Public Health. 2024;12:1320407. doi:10.3389/fpubh.2024.1320407.
- Centers for Disease Control and Prevention. Clinical overview of chickenpox (varicella). Updated July 15, 2024. https://www.cdc.gov/chickenpox/hcp/clinical-overview/index.html. Accessed May 6, 2026.
- Shu M, Zhang D, Ma R, Yang T, Pan X. Long-term vaccine efficacy of a 2-dose varicella vaccine in China from 2011 to 2021: a retrospective observational study. Front Public Health. 2022;10:1039537. doi:10.3389/fpubh.2022.1039537.
- Minhas A, Singh M, Prasad NSN, Bhardwaj A. Geospatial epidemiology of chickenpox disease in India between 2015–2021: a GIS-based analysis. Indian J Community Health. 2022;34(1):78-81. Accessed March 31, 2026.
- Perella D, Wang C, Civen R, et al. Varicella Vaccine Effectiveness in Preventing Community Transmission in the 2-Dose Era. Pediatrics. 2016;137(4):e20152802. doi:10.1542/peds.2015-2802.
- Kasi SG, Shivananda S, Marathe S, et al. Indian Academy of Pediatrics (IAP) Advisory Committee on Vaccines and Immunization Practices (ACVIP): Recommended Immunization Schedule (2020-21) and update on immunization for children aged 0 through 18 years. Indian Pediatr. 2021;58:44-53. Published online November 29, 2020. Accessed May 6, 2026. https://www.indianpediatrics.net/jan2021/jan-44-53.htm
- World Health Organization. WHO position paper on varicella vaccines – November 2025. Wkly Epidemiol Rec. 2025;100(47):567-590. Accessed May 6, 2026. https://www.who.int/publications/i/item/who-wer10047-567-590
- Varilrix, Prescribing Information, Version VRX/PI/IN/2024/01 Dated 05-September-2024. https://india-pharma.gsk.com/media/s0ehlauz/varilrix.pdf
GSK is not responsible for the third-party website content
Disclaimer
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website http://india-pharma.gsk.com/en-in/products/prescribing-information/ for full Product Information. Please report adverse events with any GSK product to the company at [email protected]. © 2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).
CL Code: PM-IN-VAR-WCNT-260007 | DOP: June 2026
For more information, please refer the following link
For Indian Healthcare Professionals Only
Key Safety Information
Contraindications:
Hypersensitivity to any active substance or excipient or neomycin. or varicella vaccine. Primary or acquired immunodeficiency who have total lymphocyte count <1200 per mm3 or other evidence of lack of cellular immune competence or subjects receiving immunosuppressive therapy (including high dose corticosteroids).
Pregnancy:
Avoid pregnancy for 1 month following vaccination.
Special warnings and precautions:
Postpone administration in acute febrile illness. Syncope (fainting) can occur following, or even before any vaccination, with adolescents, as a psychogenic reaction to injection. Avoid all contact with pregnant women susceptible to varicella (especially during first trimester pregnancy) and with high risk for developing severe varicella, especially when person vaccinated develops skin eruption within 2 to 3 weeks of immunization. To reduce infection risk of high-risk subjects, non-immune persons living in close contact with varicella patients or high-risk patients should be vaccinated. A decision should be made either to discontinue breastfeeding or to abstain from vaccination with VARILRIX, taking into account the benefit of breastfeeding for the child with regard to the benefit of prophylaxis against Varicella for the woman.
Undesirable effects: Very common- redness, pain at the injection site.
For the use only of a Registered Medical Practitioner or a Hospital or a Laboratory
Abbreviated Prescribing information of VARILRIX (Varicella Vaccine, Live IP)
ACTIVE INGREDIENT: Each 0.5 ml of the reconstituted vaccine contains: Live attenuated varicella virus (OKA strain, propagated in MRC5 human diploid cells) not less than 103.3 plaque-forming units (PFU).
INDICATION: VARILRIX is indicated for active immunisation against varicella of healthy subjects and susceptible healthy close contacts from the age of 12 months onwards. Susceptible healthy close contacts should be immunised in order to reduce the risk of transmission of virus to high-risk patients. These include parents and siblings of high-risk patients, and medical, paramedical personnel and other people who are in close contact with varicella patients or high-risk patients.
POSOLOGY AND ADMINISTRATION: Posology: The immunisation schedules for VARILRIX should be based on official recommendations. Healthy individuals: Children from 12 months of age, adolescents and adults: Children from the age of 12 months as well as adolescents and adults receive two doses of VARILRIX to ensure optimal protection against varicella. The second dose should generally be given at least 6 weeks after the first dose. Under no circumstances should the interval between the doses be less than 4 weeks. Individuals at high risk of severe varicella: Individuals at high risk of severe varicella may benefit from re-vaccination following the 2-dose schedule. Periodic measurement of varicella antibodies after immunisation may be indicated in order to identify those who may benefit from re-immunisation. Under no circumstances should the interval between the doses be less than 4 weeks. Interchangeability: A single dose of VARILRIX may be administered to subjects who have already received a single dose of another varicella-containing vaccine. A single dose of VARILRIX may be administered followed by a single dose of another varicella-containing vaccine. Method of administration: VARILRIX is to be injected subcutaneously (SC) in the deltoid region or in the anterolateral area of the thigh.
CONTRA-INDICATIONS: VARILRIX is contraindicated in individuals with severe humoral or cellular (primary or acquired) immunodeficiency such as: subjects with immunodeficiency states with a total lymphocyte count less than 1,200 per mm3; subjects presenting other evidence of lack of cellular immune competence (e.g. patients with leukaemias, lymphomas, blood dyscrasias, clinically manifest HIV infection); subjects receiving immunosuppressive therapy including high dose of corticosteroids; severe combined immunodeficiency; agammaglobulinemia; AIDS or symptomatic HIV infection or an age-specific CD4+ T-lymphocyte percentage in children below 12 months: CD4+ <25%; children between 12-35 months: CD4+ < 20%; children between 36-59 months: CD4+ < 15%. Hypersensitivity to the active substance or to any of the excipients or to neomycin. However, a history of contact dermatitis to neomycin is not a contraindication. VARILRIX is contraindicated in subjects having shown signs of hypersensitivity after previous administration of varicella vaccine. Pregnancy- Furthermore, pregnancy should be avoided for 1 month following vaccination.
SPECIAL WARNINGS and SPECIAL PRECAUTIONS: As with other vaccines, the administration of VARILRIX should be postponed in subjects suffering from acute severe febrile illness. However, the presence of a minor infection, such as a cold, should not result in the deferral of vaccination.
Syncope (fainting) can occur following, or even before any vaccination especially in adolescents as a psychogenic response to the needle injection. This can be accompanied by several neurological signs such as transient visual disturbances, paraesthesia and tonic-clonic movements during recovery. It is important that procedures are in place to avoid injury from faints. As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of a rare anaphylactic reaction following the administration of the vaccine. Alcohol and other disinfecting agents must be allowed to evaporate from the skin before injection of the vaccine since they can inactivate the attenuated viruses in the vaccine. Limited protection against varicella may be obtained by vaccination up to 72 hours after exposure to natural disease. As with any vaccine, a protective immune response may not be elicited in all vaccinees. As for other varicella vaccines, cases of varicella disease have been shown to occur in persons who have previously received VARILRIX. These breakthrough cases are usually mild, with a fewer number of lesions and less fever as compared to cases in unvaccinated individuals. Transmission: Transmission of the Oka varicella vaccine virus has been shown to occur at a very low rate in seronegative contacts of vaccinees with rash. Transmission of the Oka varicella vaccine virus from a vaccinee who does not develop a rash to seronegative contacts cannot be excluded.
Compared to healthy vaccinees, leukaemia patients are more likely to develop a papulovesicular rash. In these cases too, the course of the disease in the contacts was mild. Vaccine recipients, even those who do not develop a varicella-like rash, should attempt to avoid contact, whenever possible, with high-risk individuals susceptible to varicella for up to 6 weeks following vaccination. In circumstances where contact with high-risk individuals susceptible to varicella is unavoidable, the potential risk of transmission of the varicella vaccine virus should be weighed against the risk of acquiring and transmitting wild-type varicella virus. High-risk individuals susceptible to varicella include: Immunocompromised individuals; Pregnant women without documented positive history of varicella (chickenpox) or laboratory evidence of prior infection; Newborns of mothers without documented positive history of chickenpox or laboratory evidence of prior infection. The mild nature of the rash in the healthy contacts indicates that the virus remains attenuated after passage through human hosts. Individuals at high risk of severe varicella: There is only limited data from clinical trials available for VARILRIX (+4°C formulation) in individuals at high risk of severe varicella.
Vaccination may be considered in patients with selected immune deficiencies where the benefits outweigh the risks (e.g. asymptomatic HIV subjects, IgG subclass deficiencies, congenital neutropenia, chronic granulomatous disease, and complement deficiency diseases). Immunocompromised patients who have no contraindication for this vaccination may not respond as well as immunocompetent subjects, therefore some of these patients may acquire varicella in case of contact, despite appropriate vaccine administration. These patients should be monitored carefully for signs of varicella. Should vaccination be considered in individuals at high risk of severe varicella, it is advised that: maintenance chemotherapy should be withheld one week before and one week after immunisation of patients in the acute phase of leukaemia. Patients under radiotherapy should normally not be vaccinated during the treatment phase. Generally, patients are immunised when they are in complete haematological remission from their disease. The total lymphocyte count should be at least 1,200 per mm3 or no other evidence of lack of cellular immune competence exists. Vaccination should be carried out a few weeks before the administration of the immunosuppressive treatment for patients undergoing organ transplantation (e.g. kidney transplant). Very few reports exist on disseminated varicella with internal organ involvement following vaccination with Oka varicella vaccine strain mainly in immunocompromised subjects. VARILRIX must not be administered intravascularly or intradermally. Phenylalanine content: The vaccine contains 331 micrograms of phenylalanine per dose. Phenylalanine may be harmful for individuals with phenylketonuria (PKU).
ADVERSE EFFECTS: Very common (≥1/10): pain, erythema. Common (≥1/100 to <1/10): Rash, Pyrexia (oral / axillary temperature ≥ 37.5 °C or rectal temperature ≥ 38.0 °C)†, injection site swelling† Uncommon (≥1/1,000 to <1/100): upper respiratory tract infection, pharyngitis, lymphadenopathy, irritability, headaches, somnolence, cough, rhinitis, nausea, vomiting, viral rash, pruritus, myalgia, arthralgia, Pyrexia (oral / axillary temperature> 39.0°C or rectal temperature> 39.5°C), fatigue, malaise. Rare (≥1/10,000 to < 1/1,000): conjunctivitis, abdominal pain, diarrhea, urticaria.
According to MedDRA (Medical Dictionary for Regulatory Activities) terminology. Injection site swelling and pyrexia were reported very commonly in studies conducted in adolescents and adults. Injection site swelling was also reported very commonly after the second dose in children under 13 years of age.
Version: VRX/API/IN/2025/02 v02 dated 16-Oct-2025
Refer to full prescribing information before prescribing.
Registered medical practitioners can refer company website http://india-pharma.gsk.com/en-in/products/prescribing-information/ for full Product Information.
Please report adverse events with any GSK product to the company at [email protected]
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website: india-pharma.gsk.com/en-in/products/prescribing-information/ for Full Product Information. Please report adverse events with any GSK product to the company at [email protected]. ©2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).