
Hepatitis A Burden in the Indian Subcontinent: Emerging Vulnerability in Urbanized Populations

In this article
Summary
Key points
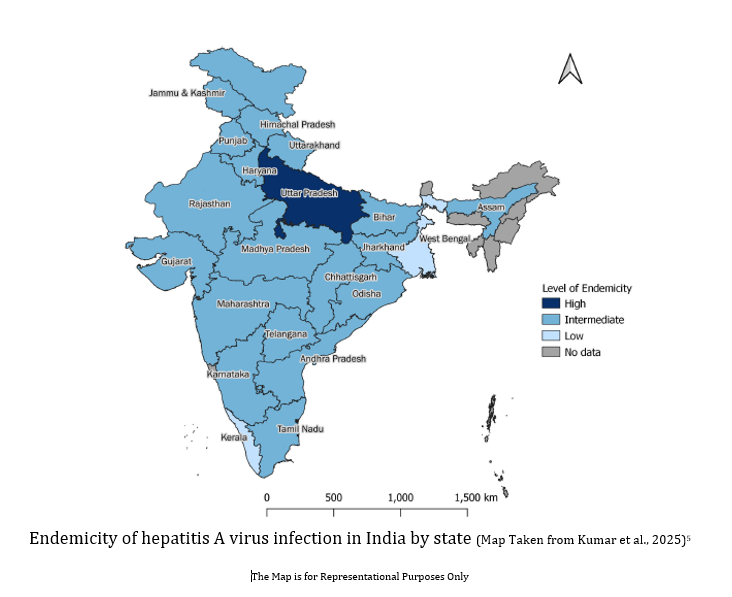
- Hepatitis A epidemiology in India is shifting from high to intermediate endemicity, driven by improved sanitation and hygiene1,2,5,6
- Reduced early-life exposure has resulted in increased susceptibility among adolescents and adults, who are more likely to develop severe disease1,2
- India contributed ~30.6 million HAV cases (95% CI: 27.7–33.4 million) and 13,658 deaths in 2021, accounting for a significant share of global disease burden5
- Surveillance data shows ~12.6% of viral hepatitis cases are due to HAV, with the majority (~74.6%) occurring in individuals <19 years5
- Seroprevalence rises with age, from ~74.7% (95% CI: 71.1–77.9) in 6–10 years to ~ 96.9% (95% CI: 96.3–97.5) in 16–30 years, indicating delayed natural immunity5
- A substantial proportion of children (~44.5% ≤15 years) remain seronegative, highlighting a large susceptible population6
- Similar susceptibility patterns in urban slum and non-slum populations indicate widespread epidemiological transition5
- The evolving disease pattern underscores the need for vaccination alongside sanitation and surveillance to reduce future burden1,2,5,6
Introduction
Hepatitis A, an acute inflammatory liver disease caused by hepatitis A virus (HAV) infection is highly endemic in the Indian subcontinent. Due to poor sanitary conditions, most of the population is exposed to the virus in childhood. Infection at this age is asymptomatic and provides life-long protection against the disease. However, due to rapid socioeconomic development and improvements in sanitation, an increasing proportion of the population is reaching adolescence and adulthood without prior exposure to HAV. Consequently, these individuals remain susceptible to infection. In contrast to childhood infections, HAV infection in older age groups is more likely to be symptomatic and is associated with an increased risk of severe complications, including acute liver failure and mortality.1
Hepatitis A virus (HAV) is a small, spherical, non-enveloped, positive-sense single-stranded RNA virus of the Picornaviridae family, classified under the Hepatovirus genus. It primarily infects the liver, leading to inflammation and jaundice.2 Although HAV can affect individuals of all ages, certain populations are at higher risk. The incubation period averages 28 days (range: 15–50 days).3 Common symptoms include abdominal pain, dark urine, clay-colored stools, diarrhea, fatigue, fever, jaundice, joint pain, loss of appetite, nausea, and vomiting.4
Epidemiology and seroprevalence of HAV
In 2021, the Global Burden of Disease Study estimated that there were 160 million (95% CI: 152-170). HAV infections globally, leading to 26,901 deaths (95% CI: 18387-42454). India accounted for 19% of the global HAV infections, with an estimated 30.6 million cases (95% CI: 27.7-33.4) and 13,658 deaths (range: 8508-24,358), contributing to nearly half of the global HAV mortality.5
Seroprevalence across urban populations stratified by socioeconomic status in Indian subcontinent
Data from northern India over a 5-year period showed an increased proportion of acute HAV infection among adults in urban settings. Subsequent studies also reported lower prior exposure to HAV among adolescents and adults in socioeconomically developed urban populations, increasing susceptibility to symptomatic infection and complications.2 Key factors associated with this epidemiologic shift include improved access to safe drinking water, hygienic sanitary practices, and changing living conditions in urbanized regions, which reduce early childhood exposure to HAV. Environmental changes affecting water availability and sanitation may also influence HAV transmission dynamics.2
- Surveillance data from India (2014–2017) showed that 12.6% of suspected viral hepatitis cases were attributable to HAV infection, with 74.6% of cases occurring in individuals aged <19 years.5
- A nationwide ICMR serosurvey (2021) demonstrated that HAV seroprevalence increased with age, from 74.7% (95% CI: 71.1–77.9) among children aged 6–10 years to 85.2% (82.7–87.4) among those aged 11–15 years and 96.9% (96.3–97.5) among individuals aged 16–30 years. Based on WHO criteria, India was categorized as having intermediate HAV endemicity.5
- The ICMR study also reported comparable seroprevalence across urban slum and non-slum populations, suggesting broader population susceptibility beyond specific socioeconomic groups.5
- In a recent multicentric study across four metropolitan Indian cities, 44.5% of individuals aged ≤15 years were anti-HAV negative and therefore susceptible to HAV infection. Pune, Chennai, and Ludhiana demonstrated intermediate endemicity, while Kolkata demonstrated low endemicity.6
- Longitudinal sero-surveillance data from Pune further demonstrated a shift from high to intermediate endemicity across both high and lower-middle socioeconomic populations over time.6

Prevention and management
Vaccination is an effective strategy for preventing hepatitis A infection and limiting transmission, and universal childhood immunization has been successfully implemented in many developed countries. However, in traditionally high-endemic countries such as India, routine universal vaccination has not been widely recommended due to early-life acquisition of natural immunity.2 With the changing epidemiology and declining seroprevalence, particularly in urban populations, a two-pronged approach is needed. First, strengthening public health measures, including improved sanitation, hygiene, and access to safe water, remains essential to reduce transmission.2 Second, vaccination remains an important preventive strategy in the context of evolving HAV epidemiology and increasing susceptibility across populations in India.2 Recent sero-epidemiological studies further highlight substantial susceptibility across both higher and lower socioeconomic populations, underscoring the need for continued surveillance and preventive strategies to reduce future disease burden.5,6
Conclusion
Hepatitis A epidemiology in the Indian subcontinent is shifting from high to intermediate endemicity, particularly in urban and higher socioeconomic populations. Reduced early childhood exposure has increased susceptibility among adolescents and adults, leading to a higher risk of symptomatic and severe disease.1,2 These trends highlight the need for strengthened surveillance and targeted vaccination strategies, alongside continued improvements in sanitation, to effectively reduce the future disease burden.1,2,5,6
Key Safety Information7
Contraindications:
HAVRIX may not be administered to persons with a known hypersensitivity to a component of the vaccine, or to those who have shown signs of hypersensitivity during a previous administration of HAVRIX.
Special warnings and precautions:
As in the case of other vaccines, HAVRIX will not be administered to patients with an acute febrile illness. A common infection does not constitute a contra-indication, however. HAVRIX may contain traces of neomycin. The vaccine will have to be used with caution in patients with a known hypersensitivity to this antibiotic. As with every product administered parenterally, it is recommended to prepare an appropriate medical treatment for immediate use, if an anaphylactic reaction were to occur. HAVRIX may be administered with persons who are HIV positive.
Undesirable Effects:
Very Common - Irritability, drowsiness, headache, pain and redness at injection site.
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory
References:
- Agrawal A, Singh S, Kolhapure S, Hoet B, Arankalle V, Mitra M. Increasing Burden of Hepatitis A in Adolescents and Adults and the Need for Long-Term Protection: A Review from the Indian Subcontinent. Infect Dis Ther. 2019;8(4):483-497. doi:10.1007/s40121-019-00270-9.
- Hussain Z, Shaikh I, Khan S, Sinh R, Patel K, Patel V. Insights of hepatitis A virus disease burden in Indian subcontinent: why urbanized localities are vulnerable to disease outbreaks? Explor Dig Dis.2025;4:100593. doi:10.37349/edd.2025.100593.
- Centers for Disease Control and Prevention. Clinical overview of hepatitis A. Updated August 29, 2025. Accessed May 16, 2026. https://www.cdc.gov/hepatitis-a/hcp/clinical-overview/index.html.
- Centers for Disease Control and Prevention. Hepatitis A surveillance—United States, 2023. Published April 15, 2025. Accessed May 16, 2026. https://www.cdc.gov/hepatitis-surveillance-2023/hepatitis-a/index.html
- Kumar MS, Kumar CPG, Saravanakumar V, et al. Seroprevalence of IgG antibodies against hepatitis-A infection among individuals aged 6-30 years in India, 2021: a nationwide population-based cross-sectional study. Lancet Reg Health Southeast Asia. 2025;41:100669. Published 2025 Sep 25. doi:10.1016/j.lansea.2025.100669.
- Lalwani S, Palkar S, Balasubramanian S, et al. Age-stratified prevalence of anti-hepatitis A virus antibodies in four metropolitan Indian cities and recent changes in Pune city. Indian J Gastroenterol. Published online March 7, 2025. doi:10.1007/s12664-025-01746-y
- Havrix, Prescribing Information, Version: HAX/PI/IN/2024/01 Dated 10-June-2024.. https://india-pharma.gsk.com/media/qqmlvec5/havrix.pdf
GSK is not responsible for the third-party website content
Disclaimer
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website http://india-pharma.gsk.com/en-in/products/prescribing-information/ for full Product Information. Please report adverse events with any GSK product to the company at [email protected]. ©2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).
CL Code: PM-IN-HAV-WCNT-260006 | DOP: June 2026
For more information, please refer the following link
For Indian Healthcare Professionals Only
Key Safety Information
Contraindications:
HAVRIX may not be administered to persons with a known hypersensitivity to a component of the vaccine, or to those who have shown signs of hypersensitivity during a previous administration of HAVRIX.
Special warnings and precautions:
As in the case of other vaccines, HAVRIX will not be administered to patients with an acute febrile illness. A common infection does not constitute a contra-indication, however. HAVRIX may contain traces of neomycin. The vaccine will have to be used with caution in patients with a known hypersensitivity to this antibiotic. As with every product administered parenterally, it is recommended to prepare an appropriate medical treatment for immediate use, if an anaphylactic reaction were to occur. HAVRIX may be administered with persons who are HIV positive.
Undesirable Effects:
Very Common - Irritability, drowsiness, headache, pain and redness at injection site
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory
Abbreviated Prescribing information of HAVRIX 1440 (ADULT) / 720 (JUNIOR)
Inactivated Hepatitis A Vaccine (Adsorbed) IP
ACTIVE INGREDIENT: HAVRIX1440: Each dose (1 ml) contains: Hepatitis A virus antigen (HAV) HM 175 strain, 1440 ELISA units (ELU); Aluminium (as aluminium hydroxide) 0.5 mg. HAVRIX720: Each dose (0.5 ml) contains: Hepatitis A virus antigen (HAV) HM 175 strain, 720 ELISA units (ELU); Aluminium (as aluminium hydroxide) 0.25 mg.
INDICATION: For active immunisation against infections caused by hepatitis A virus (HAV) for Children and Adolescents (from 1 year up to and including 18 years of age) and adults (from age 19 years and onwards). The booster dose may be given at any time between 6 months and 5 years, but preferably between 6 and 12 months after the primary dose.
DOSAGE AND ADMINISTRATION: Primary vaccination- Adults from age 19 years and onwards: A single dose of HAVRIX 1440 Adult (1.0 mL suspension) is used for primary immunisation. - Children and adolescents from 1 year up to and including 18 years of age: A single dose of HAVRIX 720 Junior (0.5 mL suspension) is used for primary immunisation. Booster vaccination- After primary vaccination with either HAVRIX 1440 Adult or HAVRIX 720 Junior, a booster dose is recommended in order to ensure long term protection. This booster dose should be given at any time between 6 months and 5 years, but preferably between 6 and 12 months after the primary dose. Method of Administration- HAVRIX must be injected intramuscularly only. It is recommended to inject the vaccine in the deltoid region in adults and in children. The deltoid muscle is not yet sufficiently developed in very young children, so the vaccine should be administered in the anterolateral part of the thigh. The injection must not be administered in the gluteal region subcutaneously or intradermally because the antibody response might be sub-optimal. However, the vaccine should be administered subcutaneously in patients suffering from thrombocytopoenia or subject to serious haemorrhage (e.g. haemophiliacs) because bleeding could occur after intramuscular administration in such persons. Strong pressure should be exercised at the site of the injection (without rubbing) for at least 2 minutes. The vaccine may never be administered intravascularly.
CONTRA-INDICATIONS: HAVRIX may not be administered to persons with a known hypersensitivity to a component of the vaccine or to those who have shown signs of hypersensitivity during a previous administration of HAVRIX.
SPECIAL WARNINGS and SPECIAL PRECAUTIONS: As in the case of other vaccines, HAVRIX will not be administered to patients with an acute febrile illness. A common infection does not constitute a contra-indication, however. People may already be in the incubation period of hepatitis A at the time of vaccination. In such circumstances, it is not certain that HAVRIX will prevent hepatitis A.
In patients undergoing haemodialysis and in subjects with a deficient immune system, the anti-HAV (hepatitis A virus) may remain insufficient after a primo-vaccination; in such patients, additional doses of the vaccine may have to be administered to attain an adequate antibody count. HAVRIX may contain traces of neomycin. The vaccine will have to be used with caution in patients with a known hypersensitivity to this antibiotic. As with every product administered parenterally, it is recommended to prepare an appropriate medical treatment for immediate use, if an anaphylactic reaction were to occur after the administration of the vaccine. For this reason, the vaccinated persons should remain under medical supervision for half an hour after vaccination. Syncope (fainting) can occur after any vaccination, or even before with adolescents in particular, as a psychogenic reaction to injection. This can be accompanied by several neurological signs such as a transient disturbance in vision, paraesthesia and tonic clonic movements of the limbs during the recovery phase. It is important that caution be set up to avoid injuries in the event of fainting. HAVRIX may be administered with persons who are HIV positive. Vaccination is not justified in subjects with anti-hepatitis A IgG.
This vaccine contains less than 1 mmol of sodium (23 mg) per dose, it is therefore essentially ‘sodium-free’. This vaccine contains potassium, less than 1 mmol (39 mg) per dose, it is therefore essentially ‘potassium-free’.
ADVERSE EFFECTS:
Clinical Trials: Frequencies, per dose, are defined as follows: Very common: ≥ 1/10, Common: ≥ 1/100 to < 1/10, Uncommon: ≥1/1000 to < 1/100, Rare: ≥1/10000 to < 1/1000, Very rare: < 1/10000.
Undesirable effects reported with HAVRIX Junior 720
Infections and infestations Uncommon: rhinitis. Metabolism and nutrition disorders Common: loss of appetite. Psychiatric disorders Very common: irritability. Nervous system disorders Common: drowsiness, headaches Very rare: neuritis, including Guillain-Barré syndrome and transverse myelitis. Gastrointestinal disorders_Common: nausea Uncommon: diarrhoea, vomiting Skin and subcutaneous tissue disorders Uncommon: rash General disorders and administrative site conditions Very common: pain and redness at injection site Common: swelling, malaise, fever (> 37.5°C) Uncommon: reaction at the injection site (induration)
Undesirable effects reported with HAVRIX 1440
Infections and infestations: Uncommon: upper respiratory tract infection, rhinitis Metabolism and nutrition disorders: Common: loss of appetite Nervous system disorders: Very common: headaches Uncommon: dizziness Rare: hypoaesthesia, paraesthesia Very rare: neuritis, including Guiliain-Barré syndrome and transverse myelitis. Gastrointestinal disorders: Common: gastrointestinal syndromes, diarrhoea, nausea Uncommon: vomiting Skin and subcutaneous tissue disorders Rare: pruritis Musculoskeletal and systemic disorders: Uncommon: myalgia, musculoskeletal stiffness General disorders and administrative site conditions: Very common: pain and redness at injection site, fatigue Common: swelling, malaise, fever (>37.5°C), reaction at the injection site (induration) Uncommon: influenza like illness Rare: shivering
Post-marketing surveillance
Immune system disorders: Anaphylactic reactions, allergic reactions, including anaphylactoid reactions and serum sickness like disease. Nervous system disorders: Convulsions Vascular disorders: Vasculitis Skin and subcutaneous tissue disorders: Angioneurotic oedema, urticaria, erythema multiforme Musculoskeletal and connective tissue disorders: Arthralgia
Version: HAX/API/IN/2025/02 v02 dated 03 Jul 2025
Registered medical practitioners can refer company website http://india-pharma.gsk.com/en-in/products/prescribing-information/ for full Product Information.
Please report adverse events with any GSK product to the company at [email protected]
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website: india-pharma.gsk.com/en-in/products/prescribing-information/ for Full Product Information. Please report adverse events with any GSK product to the company at [email protected]. ©2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).