
Revisiting pneumococcal vaccine choice Insights from the WHO SAGE & PAHO evidence-to-recommendation framework

In this article
Summary
Key points
- Pneumococcal disease is a major contributor to respiratory illness, responsible for ~30–55% of community-acquired pneumonia cases in India1
- Widespread pneumococcal vaccination has the potential to prevent >25 million cases and reduce ~407,000 deaths1
- WHO recommends that PCV10 and PCV13 are both effective in reducing invasive pneumococcal disease and pneumonia when coverage is high2
- Both 2p+1 and 3p+0 immunization schedules are effective, with selection based on programmatic feasibility and coverage2
- PCV10 demonstrates strong protection, with ~92–97% effectiveness (2+1 schedule) and additional cross-protection against serotype 19A (~71–82%)4-7
- Pneumococcal vaccination reduces hospitalizations, mortality, and overall disease burden, improving public health outcomes4-7
- Routine interchangeability between different PCV products is not recommended unless required by programmatic or epidemiological factors2
- Optimal vaccine selection should consider local serotype prevalence, epidemiology, and sustainability of immunization programs2,3
Introduction
The growing burden of pneumococcal infections, most commonly presenting as pneumonia, has become a major global public health issue. In India, the age-standardized incidence of lower respiratory tract infections (LRTIs) is estimated at 11,862 cases per 100,000 population, exceeding the regional average. Streptococcus pneumoniae is responsible for approximately 30%-55% of community-acquired pneumonia (CAP) cases among Indian adults. Although over 90 pneumococcal serotypes have been identified, invasive disease is most frequently caused by serotypes 1, 3, 5, 19F, 8, 14, 23F, 4, 19A, and 6B.1
The implementation of pneumococcal vaccination represents a crucial strategy to reduce disease burden. In India, widespread vaccine introduction has the potential to prevent more than 25 million cases, avert over 10.1 million disability-adjusted life years (DALYs), and reduce mortality by approximately 407,000 deaths.1
WHO SAGE Position Statement on PCV Use in Infants and Children Aged <5 Years2
Among infants and young children, absence of exclusive breastfeeding, malnutrition, and exposure to indoor air pollution increase the risk of bacterial pneumonia.
The incorporation of the 7-valent pneumococcal conjugate vaccine (PCV7) into childhood immunization programs beginning in 2000 resulted in a marked decline in overall invasive pneumococcal disease (IPD) incidence. Additional reductions were achieved with the subsequent introduction of the 10-valent (PCV10) and 13-valent (PCV13) pneumococcal conjugate vaccines.

Key Characteristics of the WHO-Prequalified (PCVs):
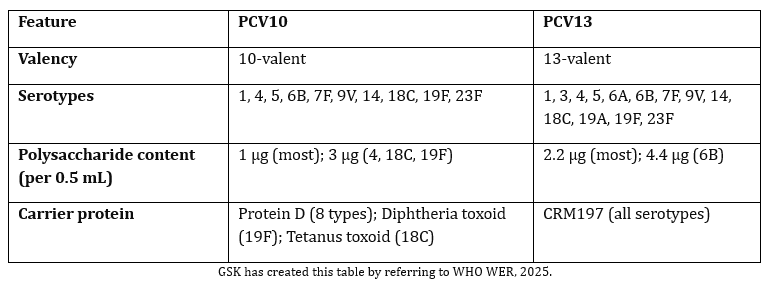
Selection of PCV Product
Current epidemiological data indicate that any of the three WHO-prequalified pneumococcal conjugate vaccines (PCV13 or PCV10), when administered with high coverage through a 3p+0 or 2p+1 infant immunization schedule, effectively controls vaccine-type invasive pneumococcal disease (IPD) and lowers the incidence of pneumococcal pneumonia in children.2
The safety and efficacy of PCV10 and PCV13 have been established across various immunization schedules, including 3p+0, 2p+1, and 3p+1, with supporting evidence from multicountry systematic reviews conducted at both global and regional levels.2
Recommendations on PCV Scheduling2,3
- Either 2p+1 or 3p+0 schedule may be used based on local context.
- First dose can be given at ≥6 weeks of age.
- 2p+1: ≥8-week interval between primary doses; booster at 9-18 months.
- Booster dose at least 6 months after the last primary dose3
- 3p+0: Maintain ≥4-week interval between doses.
Catch-Up Vaccination2
- Recommended for unvaccinated children aged 1-5 years.
- A single PCV dose is sufficient for children aged ≥24 months.*
Interchangeability of PCVs2
- No clear evidence supports interchangeability among all PCV products.
- Switching products is generally not recommended unless driven by major epidemiological, programmatic, or financial changes.
Use of Extended-Valency PCVs2
- May be considered if they better cover locally prevalent disease-causing serotypes.
Recommendations by the Pan American Health Organization (PAHO) on Pneumococcal Vaccination Strategies4
With guidance from its Strategic Advisory Group on Vaccine-Preventable Diseases, the PAHO provides the following recommendations on pneumococcal vaccine use:
- Introduce universal pneumococcal conjugate vaccines (PCV) vaccination for infants, children, immunocompromised individuals, and adults ≥65 years
- Preferred infant schedule: 2p+1 (two primary doses + booster in second year)
- If second-year coverage is low: use 3p+0 (three primary doses in first year)
- Mature programs (≥80% coverage for 5 years) may consider 1p+1 schedule; aim for ≥90% national coverage
- Ensure ≥90% final-dose coverage with ≥80% municipal-level homogeneity
- Reintroduce PCV with 2p+1 schedule in low-coverage or interrupted programs (or 3p+0 if needed)
- Select PCV valency based on local serotype epidemiology, replacement patterns, and program sustainability
- Adults ≥65 years and high-risk groups: consider one dose of PCV20
- Fractional dosing is not recommended for higher-valency PCVs
In line with these recommendations, the Indian Academy of Paediatrics (IAP) advices a 3+1 PCV schedule for infants. This includes a primary series at 6, 10 and 14 weeks given alongside routine immunizations, followed by a booster dose at 12-15 months to complete the schedule.5
Evidence on PCV10 Effectiveness6-9
PCV10 has demonstrated strong effectiveness against vaccine-type invasive pneumococcal disease (IPD) in children ≤5 years of age. Reported vaccine effectiveness ranges from 72.8%-100% with the 3+1 schedule and 92%-97% with the 2+1 schedule. Significant cross-protection against serotype 19A (82.2% and 71%) has also been observed. In addition, PCV10 has shown effectiveness against both clinically defined and bacteriologically confirmed acute otitis media, supporting its role in reducing overall pneumococcal disease burden.
Beyond disease-specific outcomes, PCV10 vaccination has been associated with reductions in pneumonia-related hospitalizations, pneumonia mortality, and all-cause mortality. Economic evaluations further indicate that PCV10 improves cost-effectiveness and increases quality-adjusted life years compared with no vaccination.
Conclusion
Pneumococcal disease remains a significant cause of morbidity and mortality, particularly in young children and older adults. Evidence from WHO SAGE and PAHO affirms that any WHO-prequalified PCV, when administered with high coverage through recommended schedules, effectively reduces IPD and pneumococcal pneumonia. Sustained high vaccination coverage and context-specific vaccine selection are essential to achieving long-term disease control and population-level protection.
*children aged 12months-5 years: The vaccination schedule consists of two doses of 0.5ml with an interval of atleast 2 months between doses.3
Key Safety Information3
Contraindications
Hypersensitivity to the active substances or to any of the excipients listed in section 2. Qualitative and Quantitative Composition or to any of the carrier proteins.
As with other vaccines, the administration of SYNFLORIX should be postponed in subjects suffering from acute severe febrile illness. However, the presence of a minor infection, such as a cold, should not result in the deferral of vaccination.
Adverse Effects
The most common adverse reactions observed after primary vaccination were redness at the injection site and irritability which occurred after approximately 41% and 55% of all doses respectively. Following booster vaccination, children >12 months of age are more likely to experience injection site reactions compared to the rates observed in infants during the primary series with SYNFLORIX In comparative clinical studies, the incidence of local and general adverse events reported within 4 days after each Synflorix dose was within the same range as after vaccination with PCV 7. The majority of these reactions were of mild to moderate severity and were not long lasting
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory
References
- Rao CR, Kamath VG, Nadda A, et al. IAPSM's Position Paper on Pneumococcal Vaccine (PCV) for Adult Immunization in India. Indian J Community Med. 2024;49(Suppl 2):S132-S138. doi:10.4103/ijcm.ijcm_739_24
- WHO. WHO position paper: Pneumococcal conjugate vaccines in infants and children aged <5 years – September 2025. Weekly Epidemiological Record. 26 September 2025;100(39):411–438.
- Synflorix, Abbreviated Prescribing Information, Version: SYN/API/IN updated on 29 July 2025. https://india-pharma.gsk.com/media/z33hpz0v/synflorix.pdf
- Recommendations for pneumococcus. Pan American Health Organization. 2026. https://www.paho.org/sites/default/files/2026/02/recommendations-pneumococcus-2026.pdf . Accessed on 03 June, 2026
- Pai UA, Kasi S, Patel N, Narayanan V. Pneumococcal conjugate vaccines in India: reviewing disease burden, serotypes, vaccine choice and dosing schedules. Asian J Pediatr Res. 2025;15(3):433-? doi:10.9734/ajpr/2025/v15i3433.
- Berman-Rosa M, O'Donnell S, Barker M, Quach C. Efficacy and Effectiveness of the PCV-10 and PCV-13 Vaccines Against Invasive Pneumococcal Disease. Pediatrics. 2020;145(4):e20190377. doi:10.1542/peds.2019-0377
- World Health Organization Strategic Advisory Group of Experts (SAGE) on Immunization. Pneumococcal Conjugate Vaccine (PCV) Review of Impact Evidence (PRIME): Summary of Findings from Systematic Review. October 2017.
- Vo NX, Pham HL, Bui UM, Ho HT, Bui TT. Cost-effectiveness analysis of pneumococcal vaccines in the pediatric population: a systematic review. Healthcare (Basel). 2024;12(19):1950. doi:10.3390/healthcare12191950.
- Diaz J, Terrazas S, Bierrenbach AL, et al. Effectiveness of the 10-Valent Pneumococcal Conjugate Vaccine (PCV-10) in Children in Chile: A Nested Case-Control Study Using Nationwide Pneumonia Morbidity and Mortality Surveillance Data. PLoS One. 2016;11(4):e0153141. Published 2016 Apr 8. doi:10.1371/journal.pone.0153141
GSK is not responsible for the third-party website content
Disclaimer
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website http://india-pharma.gsk.com/en-in/products/prescribing-information/ for full Product Information. Please report adverse events with any GSK product to the company at [email protected] 2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).
CL Code: PM-IN-SYN-WCNT-260001 | DOP: June 2026
For more information, please refer the following link
For Indian Healthcare Professionals Only
Key Safety Information
Contraindications
Hypersensitivity to the active substances or to any of the excipients listed in section 2. Qualitative and Quantitative Composition or to any of the carrier proteins.
As with other vaccines, the administration of SYNFLORIX should be postponed in subjects suffering from acute severe febrile illness. However, the presence of a minor infection, such as a cold, should not result in the deferral of vaccination.
Adverse Effects
The most common adverse reactions observed after primary vaccination were redness at the injection site and irritability which occurred after approximately 41% and 55% of all doses respectively. Following booster vaccination, children >12 months of age are more likely to experience injection site reactions compared to the rates observed in infants during the primary series with SYNFLORIX In comparative clinical studies, the incidence of local and general adverse events reported within 4 days after each Synflorix dose was within the same range as after vaccination with PCV 7. The majority of these reactions were of mild to moderate severity and were not long lasting
For the use only of Registered Medical Practitioners or a Hospital or a Laboratory
Abbreviated Prescribing information of SYNFLORIX [Pneumococcal Polysaccharide Conjugate Vaccine (adsorbed) IP]
ACTIVE INGREDIENT: One dose (0.5 ml) contains 1 microgram of polysaccharide for serotypes 11,2, 51,2, 6B1,2, 7F1,2, 9V1,2, 141,2 and 23F1,2, and 3 micrograms of serotypes 41,2, 18C1,3 and 19F1,4.
1 adsorbed on aluminium phosphate 0.5 milligram Al3+
2 conjugated to protein D (derived from non-Typeable Haemophilus influenzae) carrier protein 9-16 micrograms
3 conjugated to tetanus toxoid carrier protein 5-10 micrograms
4 conjugated to diphtheria toxoid carrier protein 3-6 micrograms
INDICATION: Active immunisation of infants and children from 6 weeks up to 5 years of age against disease caused by 10 serotypes of Streptococcus pneumoniae i.e serotypes 1, 4, 5, 6B, 7F, 9V, 14, 18C, 19F, 23F and cross-reactive serotype 19A (including sepsis, meningitis, pneumonia, bacteraemia and acute otitis media) and against acute otitis media caused by Non-Typeable Haemophilus influenzae.
DOSAGE AND ADMINISTRATION: Posology: The immunization schedules for SYNFLORIX should be based on official recommendations. Infants from 6 weeks to 6 months of age: Three-dose primary series - The recommended immunization series to ensure optimal protection consists of four doses, each of 0.5 ml. The primary infant series consists of three doses with the first dose usually given at 2 months of age and with an interval of at least 1 month between doses. The first dose may be given as early as 6 weeks of age. A booster (fourth) dose is recommended at least 6 months after the last primary dose (preferably between 12 and 15 months of age). Two-dose primary series - Alternatively, when SYNFLORIX is given as part of a routine infant immunization program, a series consisting of three doses, each of 0.5 ml may be given. The first dose may be given as early as 6 weeks of age with a second dose administered 2 months later. A booster (third) dose is recommended at least 6 months after the last primary dose (preferably between 12 and 15 months of age). Preterm newborn infants (born between 27-36 weeks gestation): In preterm infants born after at least 27 weeks of gestational age, the recommended immunization series consists of four doses, each of 0.5 ml. The primary infant series consists of three doses with the first dose given at 2 months of age and with an interval of at least 1 month between doses. A booster (fourth) dose is recommended at least 6 months after the last primary dose. Unvaccinated infants and children ≥ 7 months of age: infants aged 7-11 months: The vaccination schedule consists of two primary doses of 0.5 ml with an interval of at least 1 month between doses. A booster (third) dose is recommended in the second year of life with an interval of at least 2 months after the last primary dose. Children aged 12 months – 5 years: The vaccination schedule consists of two doses of 0.5 ml with an interval of at least 2 months between doses. It is recommended that subjects who receive a first dose of SYNFLORIX complete the full vaccination course with SYNFLORIX. Special populations: In individuals who have underlying conditions predisposing them to invasive pneumococcal disease (such as Human Immunodeficiency Virus (HIV) infection, sickle cell disease (SCD) or splenic dysfunction) SYNFLORIX may be given according to the above-mentioned schedules except that a 3-dose schedule should be given as primary vaccination in infants starting vaccination before 6 months of age. Paediatric population: The safety and efficacy of SYNFLORIX in children over 5 years of age have not been established. Method of Administration: The vaccine should be given by intramuscular injection. The preferred sites are anterolateral aspect of the thigh in infants or the deltoid muscle of the upper arm in young children.
CONTRA-INDICATIONS: Hypersensitivity to the active substances or to any of the excipients or to any of the carrier proteins. As with other vaccines, the administration of SYNFLORIX should be postponed in subjects suffering from acute severe febrile illness. However, the presence of a minor infection, such as a cold, should not result in the deferral of vaccination.
SPECIAL WARNINGS and PRECAUTIONS: As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of a rare anaphylactic reaction following the administration of the vaccine. The potential risk of apnoea and the need for respiratory monitoring for 48-72h should be considered when administering the primary immunization series to very premature infants (born ≤ 28 weeks of gestation) and particularly for those with a previous history of respiratory immaturity. As the benefit of vaccination is high in this group of infants, vaccination should not be withheld or delayed. SYNFLORIX should under no circumstances be administered intravascularly or intradermally. No data are available on subcutaneous administration of SYNFLORIX. In children as of 2 years of age, syncope (fainting) can occur following, or even before, any vaccination as a psychogenic response to the needle injection. It is important that procedures are in place to avoid injury from faints. As for other vaccines administered intramuscularly, SYNFLORIX should be given with caution to individuals with thrombocytopenia or any coagulation disorder since bleeding may occur following an intramuscular administration to these subjects. Official recommendations for the immunization against diphtheria, tetanus and Haemophilus influenzae type b should also be followed. There is insufficient evidence that SYNFLORIX provides protection against pneumococcal serotypes not contained in the vaccine except the cross-reactive serotype 19A. SYNFLORIX does not provide protection against other micro-organisms. As with any vaccine, SYNFLORIX may not protect all vaccinated individuals against invasive pneumococcal disease, pneumonia or otitis media caused by the serotypes in the vaccine and the cross-reactive serotype 19A. In addition, as otitis media and pneumonia are caused by many micro-organisms other than the Streptococcus pneumoniae serotypes represented by the vaccine, the overall protection against these diseases is expected to be limited and substantially lower than protection against invasive disease caused by the serotypes in the vaccine and serotype 19A. In clinical trials SYNFLORIX elicited an immune response to all ten serotypes included in the vaccine, but the magnitude of the responses varied between serotypes. The functional immune response to serotypes 1 and 5 was lower in magnitude than the response against all other vaccine serotypes. It is not known whether this lower functional immune response against serotypes 1 and 5 will result in lower protective efficacy against invasive disease, pneumonia or otitis media caused by these serotypes. Children should receive the dose regimen of SYNFLORIX that is appropriate to their age at the time of commencing the vaccination series Safety and immunogenicity data are not yet available in children above 5 years of age. Children with impaired immune responsiveness, whether due to the use of immunosuppressive therapy, a genetic defect, HIV infection, prenatal exposure to anti-retroviral therapy and/or to HIV, or other causes, may have reduced antibody response to vaccination. Safety and immunogenicity data are available for HIV infected infants (asymptomatic or with mild symptoms according to WHO classification), HIV negative infants born from HIV positive mothers, children with sickle cell disease and children with splenic dysfunction. Safety and immunogenicity data for SYNFLORIX are not available for individuals in other specific immunocompromised groups and vaccination should be considered on an individual basis. Children younger than 2 years old should receive the appropriate-for-age SYNFLORIX vaccination series. The use of pneumococcal conjugate vaccine does not replace the use of 23-valent pneumococcal polysaccharide vaccines in children ≥ 2 years of age with conditions (such as sickle cell disease, asplenia, HIV infection, chronic illness, or those who have other immunocompromising conditions) placing them at higher risk for invasive disease due to Streptococcus pneumoniae. Whenever recommended, children at risk who are ≥ 24 months of age and already primed with SYNFLORIX should receive 23-valent pneumococcal polysaccharide vaccine. The interval between the pneumococcal conjugate vaccine (SYNFLORIX) and the 23-valent pneumococcal polysaccharide vaccine should not be less than 8 weeks. There are no data available to indicate whether the administration of pneumococcal polysaccharide vaccine to SYNFLORIX primed children may result in hyporesponsiveness to further doses of pneumococcal polysaccharide or to pneumococcal conjugate vaccine. Prophylactic administration of antipyretics before or immediately after vaccine administration can reduce the incidence and intensity of post-vaccination febrile reactions. Clinical data generated with paracetamol and ibuprofen suggest that the prophylactic use of paracetamol might reduce the fever rate, while prophylactic use of ibuprofen showed a limited effect in reducing fever rate. The clinical data suggests that paracetamol might reduce the immune response to SYNFLORIX. However, the clinical relevance of this observation is not known. The use of prophylactic antipyretic medicinal products is recommended: i. For all children receiving SYNFLORIX simultaneously with vaccines containing whole cell pertussis because of higher rate of febrile reactions. ii. For children with seizure disorders or with a prior history of febrile seizures. Antipyretic treatment should be initiated according to local treatment guidelines.
ADVERSE EFFECTS: Frequencies are reported as: Very common (≥ 1/10), Common (≥1/100 to <1/10), Uncommon (≥1/1,000 to <1/100), Rare (≥1/10,000 to <1/1,000), Very rare (<1/10,000).
Clinical trials: Very common: Appetite lost, Irritability, Drowsiness, Pain, redness, swelling at the injection site, fever ≥38°C rectally (age < 2 years). Common: Injection site reactions like injection site induration, fever >39°C rectally (age < 2 years). Uncommon: Crying abnormal, Apnoea in very premature infants (≤28 weeks of gestation), Diarrhoea, vomiting, Rash, Injection site reactions like injection site haematoma, haemorrhage and nodule. Rare: Allergic reactions (such as allergic dermatitis, atopic dermatitis, eczema), Convulsions (including febrile convulsions), Urticaria. Very rare: Angioedema, Kawasaki disease.
Adverse reactions additionally reported after booster vaccination of primary series and/or catch-up vaccination: Common: Fever ≥38°C rectally (age 2 to 5 years). Uncommon: Headache (age 2 to 5 years), Nausea (age 2 to 5 years), Injection site reactions like pruritus, fever > 40°C rectally (age < 2 years), fever >39°C rectally (age 2 to 5 years), diffuse swelling of the injected limb, sometimes involving the adjacent joint.
Post-marketing experience: Rare: Hypotonic-hyporesponsive episode. Very rare: Anaphylaxis.
Version: SYN/API/IN updated on 29 July 2025
Registered medical practitioners can refer company website http://india-pharma.gsk.com/en-in/products/prescribing-information/ for full Product Information.
Please report adverse events with any GSK product to the company at [email protected]
For the use only of a registered medical practitioner or a hospital or a laboratory. Trademarks are owned by or licensed to the GSK group of companies. Refer to full prescribing information before use. Registered medical practitioners can refer company website: india-pharma.gsk.com/en-in/products/prescribing-information/ for Full Product Information. Please report adverse events with any GSK product to the company at [email protected]. ©2026 GSK group of companies or its licensor. For more information, please contact: GlaxoSmithKline Pharmaceuticals Limited, Dr. Annie Besant Road, Worli, Mumbai – 400030 (India).